by Karin Chernoff Kaplan, Managing Director
Open PDF file >
Why It’s Time to Update Your Physician Compensation Model
It’s time to stop playing “kick the can” when it comes to physician compensation in hospitals and health systems.
When the 2021 Medicare Physician Fee Schedule (MPFS) sought to restructure physician reimbursement by increasing payment to cognitive care specialists such as primary care physicians and reducing reimbursement for procedure-based specialists, it was a move designed to strengthen investment in primary care and chronic disease management. These are specialties that historically have been under-reimbursed.
The coronavirus relief package passed at the end of 2020 included 3.75 percent more reimbursement for physicians than originally intended. This effectively mitigated the impact of the 2021 MPFS on procedure-based physicians. It also resulted in even better-than-expected reimbursement for cognitive specialists.
For hospitals and health systems—many of which base physician compensation on the work relative value unit (wRVU) values published in the MPFS as a neutral way of measuring physician productivity—substantial changes to the MPFS held the unintended potential to wreak havoc on physician compensation plans. In some organizations—such as those that compensate cognitive physicians on a pay-per-RVU basis—primary care physicians alone could have seen a 20% increase in compensation for the same services. It was an increase many organizations couldn’t have withstood, especially in the middle of a pandemic.
As a result, many hospital and health system leaders effectively said, “We’re going to stick with the 2020 MPFS wRVU values for now for the purposes of determining compensation.”
But organizations can’t stick with the 2020 values forever. Instead, leaders need to do the hard work of determining their physician compensation philosophy for 2022 and beyond. It’s a scenario we’re seeing at organizations across the country as leaders revisit their compensation models to ensure that they are both fair and financially sustainable.
Determining Your Compensation Philosophy
There are four questions that can help guide leaders’ efforts to determine their physician compensation philosophy in 2022.
- Will we increase compensation for cognitive specialists—and if so, how?
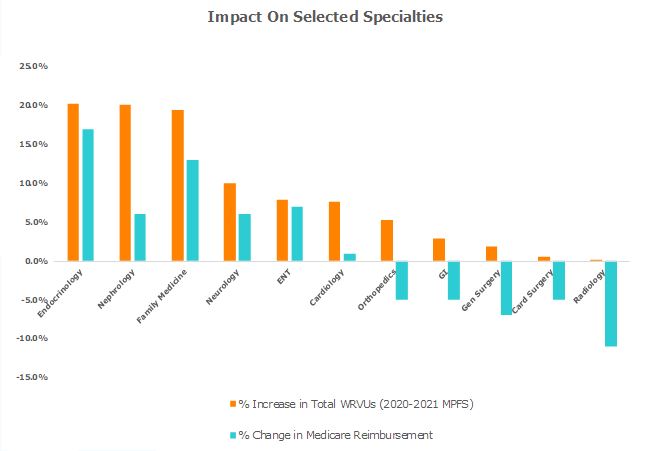
Do leaders agree that cognitive specialists have historically been undervalued and that compensation should be adjusted to reflect their importance in detecting and managing complex disease—efforts that improve outcomes and reduce costs of care and the strain on system resources? If so, will this increase be applied on a per-RVU basis, and if so, at what rate (e.g., the 2022 MPFS rate for cognitive specialists or an organization-specific RVU threshold)? Or, is now the time to explore a non-work RVU model?Ultimately, this decision will come down to what actions the organization can afford to take. Given that the impact of applying the 2021 MPFS RVUs could have resulted in a 20 percent increase in compensation for family medicine physicians and endocrinologists (see the table below), leaders who agree that an increase in compensation is needed may wish to adopt an alternative approach to avoid breaking the bank. Now might also be the time to revisit whether a work RVU-based physician model still meets the organization’s needs or whether this model is outdated in the current environment.It’s important to note that the changes in reimbursement resulting from the MPFS only apply to Medicare reimbursement. Among commercial payers, similar changes to reimbursement are not in store—at least not immediately.
- If we increase compensation for cognitive specialists, will we decrease compensation for procedure-based specialists? No one wants to walk into a room of physicians and tell them they will be paid less for doing the same work, even if this could happen in private practice. Doing so could spark significant backlash among procedure-based specialists, particularly if no one else in the market is cutting procedural specialists’ pay. It’s one reason why legislators continue to put off the decrease in reimbursement for procedure-based specialists: It’s a politically unpopular move, especially during a pandemic.
- If we reevaluate RVU thresholds or our pay per RVU, which data will we use? Consider that the current physician productivity data are at least a year old (e.g., a 2021 MGMA report will be based on 2020 data). Further, physician productivity data are skewed by the pandemic, since some specialists were busier than others during the first year of the pandemic. It will take a few years for market data to catch up to the current operating environment. As a result, leaders will need to proactively take a stand on how their organization will set physician compensation levels for 2022 and beyond, without the ability to rely on precise market data to guide or justify their approach.
- What impact will your decision have on recruitment and retention? Today, physicians are leaving the profession at a rate that is four times higher than before the pandemic. Some specialists—such as primary care physicians—also are a prime target for private equity investor recruitment. Your organization’s physician compensation philosophy must consider: “What will it take for our organization to remain competitive in our market?”
Now is the time for hospital and health system leaders to convene a work group to establish the right compensation philosophy and approach for 2022 and beyond.
Contact the Author:
Karin Chernoff Kaplan, Managing Director, kkaplan@veralon.com