by Karin Chernoff Kaplan, Managing Director
and Kelvin Polanco, Manager
Open PDF file >
Where Have All the Anesthesia Specialists Gone? Insights for Healthcare Leaders
Anesthesia provider shortages aren’t new, and they aren’t limited to certain geographic regions, but they are getting worse—and it’s time to consider new responses.
By 2033, the shortage of anesthesiologists nationwide is expected to reach 12,500, according to an often-cited American Association of Medical Colleges (AAMC) report. From 2016 to 2021, the number of anesthesiologists increased just 1.1%, while the number of physicians across all specialties increased 7%. Meanwhile, among certified registered nurse anesthetists (CRNAs), the shortage could reach 7,800 by 2028.
Why?
- Growth, Aging & Decline in Health of Population: Between 2000 and 2020, the U.S Population grew 18%, while the overall surgery volume increased 31.5%. Population growth was (and is projected to be) most significant in the population over aged 65, the highest users of health care services.
- Aging of Anesthesiologists: Baby boomers (Aged 57-75) dominate anesthesia, representing 37.6% of the active members of the American Society of Anesthesiologists (ASA), but only 27% of the U.S workforce. Gen X (Aged 45-56) are underrepresented, accounting for 29.5% of the ASA, while 35% are in the U.S workforce.[1]
- Residency Slots: Between 2016 and 2021, the number of first-year anesthesia residents and fellows has only increased from 1,760 to 1,863, only a 103-slot improvement.[2] Anesthesia is the third hardest hospital-based specialty to match into as a medical student, with 10.5% of applicants not finding a job.[3]
- More Anesthetizing Locations: Sedation has expanded outside the operating room (OR) to endoscopy labs, cardiac catheterization labs, ambulatory services centers (ASCs), requiring more providers to provide care.
As a result, CRNAs have become a popular alternative to anesthesiologists: They are less expensive than anesthesiologists, and multiple research studies have failed to demonstrate a difference in safety between the two groups. Today, many hospitals are leaning on CRNAs to cut costs in the wake of the pandemic.
Comparing Compensation Between Anesthesiologists and CRNAs
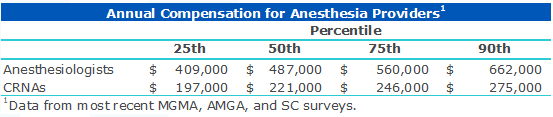
But as the low supply of anesthesiologists demands alternative options for care, healthcare leaders must consider whether the actions they have taken today are working and how to respond as shortages increase.
Combating the Shortage in Anesthesia Specialists
Amid declining options for securing anesthesia coverage, large companies—from NorthStar Anesthesia to TeamHealth to U.S. Anesthesia—have emerged to provide anesthesia care. Many of these companies are private-equity backed, resulting in cost increases and a hyper focus on profitability. The Federal Trade Commission has said it considers private equity backed consolidations to be an enforcement priority.
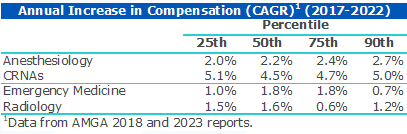
In this environment, compensation increases for anesthesia providers, in particular for CRNAs, outpaced compensation increases for anesthesiologists and other hospital-based providers.
Provider Shortages Put Pressure on Compensation
To combat the shortage in anesthesiologists, the federal government enabled states to opt out of physician supervision requirements for CRNAs, essentially making it possible for CRNAs to provide care on their own to fill hospital gaps in anesthesia needs. Twenty-six states have followed suit, particularly rural states that face challenges convincing anesthesiologists to work exclusively at small-budget, rural hospitals. Not surprisingly, it’s a move that anesthesiologists aren’t happy with, as they believe CRNAs aren’t qualified to take on this level of responsibility for care.
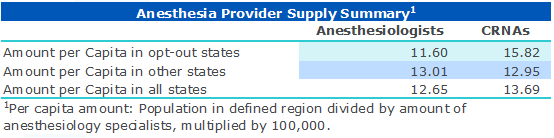
So how has this strategy worked? A data analysis suggests there’s a relationship between the number of CRNAs and anesthesiologists in opt-out states than other states, with a higher proportion of CRNAs in opt-out states and more anesthesiologists in other states.
The Impact of the “Opt-Out” Option on State-by-State Anesthesiology Coverage
States that haven’t opted out likely will face pressure to do so, given the considerably lower cost of hiring CRNAs versus anesthesiologists, and the impact such a move would make on CRNA availability statewide.
But there’s a risk to relying heavily on CRNAs versus anesthesiologists. In addition to the lower level of training that CRNAs bring to the table, and as shown above, compensation for CRNAs is increasing at a faster rate than for other specialty providers. Moreover, hospitals and health systems may feel pressure to hire anesthesiologists or acquire anesthesiology practices to keep specialized talent on board.
Key Actions for Leaders
What actions should healthcare leaders take to shore up anesthesia coverage in a resource-constrained and highly competitive environment? Here are four considerations.
- Encourage nurses to become CRNAs. The low supply of anesthesiologists creates high demand for anesthesia care that will only get worse as baby boomers age, well-capitalized anesthesiology companies acquire top talent, and more surgical care shifts to outpatient settings. Given that CRNAs must have nursing degrees, offering incentives for nurses to pursue this occupation—with guarantee of higher pay once they have earned their degree—could help provide a base of CRNA talent for hospitals and health systems that will help them weather anesthesiologist shortages down the road.
- Take a look at anesthesia staffing ratios with an eye toward expense reduction. Examine opportunities to safely reduce anesthesiologist coverage in favor of CRNAs to reduce costs without sacrificing quality of care. Although state law may limit the extent of CRNA utilization, research and practical application of data suggests that the potential for cost savings in staffing an anesthesia service line increases as CRNA utilization increases. Medical staff bylaws or medical staff culture may be a barrier to modification of the staffing models.
- Consider whether employment of anesthesiologists could help your organization better control staffing and costs. Historically, many hospitals have contracted with outside anesthesia groups to provide care, typically with subsidies built in. One emerging approach Veralon is seeing hospitals take is to offer employment to these groups, which helps avoid continued growth in subsidies and gives hospitals greater control over their anesthesia care staffing and costs. As anesthesiologists nationwide consider offers of employment from large supergroup contractors, smaller anesthesia groups may be seeking conversion to employment. Hospital and health system leaders should consider whether their organization is open to employment, the value this could provide, and the terms they would be willing to offer to protect long-term coverage. In doing so, hospital leaders will want to make offers that consider work life balance to minimize burnout including: defined work shifts, job sharing, access to CME, flexible hours, and of course competitive compensation.
- If anesthesia is provided under a PSA, consider creative solutions including at-risk dollars for achieving administrative/operational goals, such as staffing models which include CRNAs or clinical quality goals similar to those found in co-management arrangements.
By taking a close look at their organization’s anesthesia staffing needs, now and in the future, healthcare leaders can thoughtfully consider the extent to which they should invest in these and other approaches to make sure patients can receive the care they need, when and where they need it.
[1] “The Future of Anesthesiology: How Anesthesiologist and CRNA Shortages Are Making an Impact.” (n.d.). Retrieved from: https://mbmps.com/the-future-of-anesthesiology-how-anesthesiologist-and-crna-shortages-are-making-an-impact/
[2] “2022 Physician Specialty Date Report – Table 2.6: Percentage Change in Number of First-Year ACGME Residents and Fellows by Specialty, 2016-2021. Retrieved from: https://www.aamc.org/data-reports/workforce/data/percentage-change-first-year-acgme-residents-fellows-specialty-2016-2021
[3] “2022 Main Residency Match ® Results and Data Report”. Retrieved from: https://www.nrmp.org/wp-content/uploads/2022/05/2022-Main-Match-Results-and-Data_Final.pdf
Contact the Authors:
Karin Chernoff Kaplan, Managing Director, kkaplan@veralon.com
Kelvin Polanco, Manager, kpolanco@veralon.com