by Idette Elizondo and Andrew Isdaner
Open PDF file >
Getting Ready for CJR
If your hospital is in one of the 67 regions affected by the Comprehensive Care for Joint Replacement (CJR) program, you probably are wondering what you can do to prepare. The program will start on April 1, 2016.
The good news is that because there is a tremendous amount of similarity between the CJR and Bundled Payment for Care Improvement (BPCI) initiatives, there is a lot to be learned from the providers who have been successful in BPCI bundles for Major Joint.
Similarities and Differences
Both initiatives include:
- Patients with Medicare Part A&B
- A retrospective payment model that looks at how costs compare to historical costs
- Gainsharing on both internal costs and episode costs
- Similar waivers for 3-day stay, telehealth, and home health direct supervision
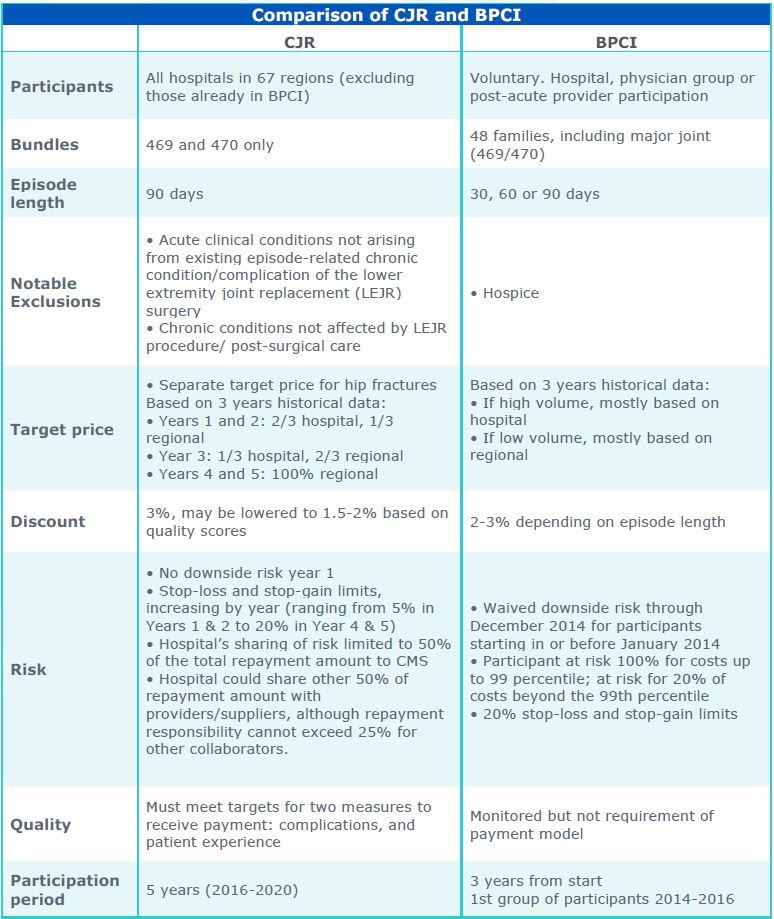
The primary differences in the CJR model are:
- There is no choice of bundle length—90-day bundles are required
- The target price is based more heavily on regional cost averages, putting more cost pressure on organizations with above-average costs
- Payments are contingent on meeting specified quality performance targets
The differences are delineated in the table below.
Where to Start
We know that hospitals that have been successful in BPCI for Major Joint have succeeded by reducing costs in the post-acute stage of the episode. That will only become more important with a mandated 90-day episode. Hospitals have had some luck at managing which type of setting patients go to immediately after post-acute care, but have had more difficulties in lowering length of stay for patients that go to SNFs. That should be a first target for providers in the CJR program.
The second target is the process of setting patient expectations for post-acute care, even prior to hospitalization, and certainly early in the acute care stay. Patients need to understand that it may be entirely appropriate for them to take a different post-acute path than that of friends who have had the same procedure. That reduces pressure on physicians and lowers the time to post-acute placement.
Finally, it’s important to change the way patients are managed during their hospital stay—the actual model of clinical care. Not only does this have the potential to shorten the length of the acute care stay with better patient outcomes, it can also allow a shorter stay or less intense level of post-acute care.