by Karin Chernoff Kaplan, Managing Director
Open PDF file >
Don’t Forget the Second Wave of WRVU Changes
The First Wave
2021 was the big year for WRVU changes associated with CMS’s extensive and far-reaching updates to the Medicare Physician Fee Schedule (MPFS). The changes, designed to ultimately be budget neutral, restructured reimbursement to increase payments to cognitive specialists (such as primary care and other medical specialties) and reduce reimbursement to procedure-based specialists.
These goals were accomplished primarily through two changes:
- Changes to the Work RVUs (WRVUs) assigned to individual CPT codes – most notably, increased WRVUs assigned to the E&M CPT codes which represent the largest source of revenue for cognitive specialties; and
- Reduction in the conversion factor (which determines payment levels).
Since then, health systems have been challenged with the impact of the WRVU changes on their productivity-based compensation plans. Further, the changes wreaked havoc on the market data i.e., the surveys, which most health systems and compensation professionals rely on in evaluating and determining provider compensation.
The Second Wave
Many professionals thought disruption to the market data and compensation plans was behind us and that the more reliable market data, which would reflect compensation (and WRVUs) under the new fee schedule, was around the corner. But CMS issued a final rule that included additional updates and policy changes to the MPFS effective January 1, 2023.
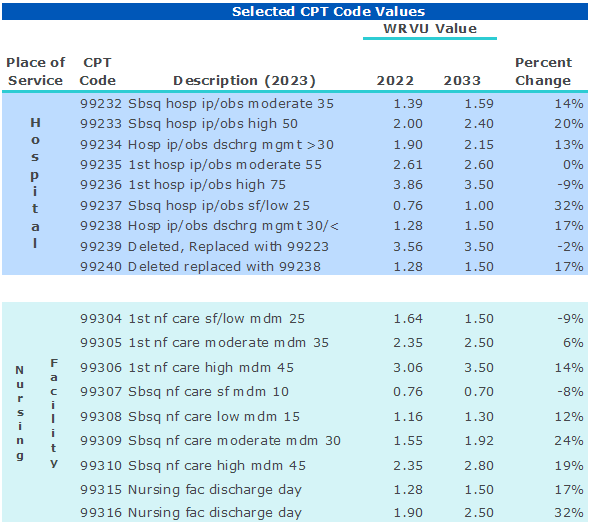
The 2023 MPFS includes statutory budget neutrality adjustments, and, similar to the approach finalized in the 2021 change with regard to outpatient E&M codes, an overall increase in work Relative Value Units for evaluation and management (E&M) services in hospitals and nursing facilities. Table 1 includes the most commonly used E&M codes WRVUs in hospitals and nursing facilities and the associated WRVU changes.
Table 1
The extent to which the WRVU changes will impact individual providers depends on the extent to which providers see patients in the hospital (or nursing facility) setting and whether they are on WRVU based compensation model. We know that a material portion of inpatient hospital care is provided by hospitalists. Veralon reviewed national utilization data for hospitalists to estimate the potential impact on WRVUs. Based on this analysis, a typical hospitalist will generate 11 percent more WRVUs for the same number of hospital visits. This will flow directly to compensation under a productivity-based model.
Other specialists that provide a portion of their total basket of services in the hospital or nursing facility setting will be impacted as well. Providers in the post-acute setting paid based on WRVUs, may, without mitigation, see material increases in compensation.
We note that while not included in Table 1 above, CMS also made changes to the codes associated with home visits.
Health systems, (and other employers utilizing WRVUs in compensation plans) should be aware of the impact of the changes in the MPFS on provider compensation plans for specialties most likely to be affected.
Contact the Author:
Karin Chernoff Kaplan, Managing Director, kkaplan@veralon.com