by Karin Chernoff Kaplan, Managing Director
Open PDF file >
Determining Compensation for Super-Specialized Physicians: What to Consider
Before the early 20th century, there were virtually no physician specialists in the United States. Today, the list of physician specialties continues to expand as medical knowledge grows with new discoveries and advancements in technology.
Now, healthcare leaders must consider: How does this super-specialization affect physician compensation?
Specialization and Sub-Specialization
Historically, physicians were generalists, but many forces over the centuries shaped their gradual evolution into specialists. The first residencies were established in 1927, and in the 1930s, 13 medical specialties were recognized, and specialty boards were established to certify specialists.
Driven by the evolution of population health needs, medical advances, the identification of new diseases and, in some cases, pure economics, new specialties and subspecialties continue to emerge. Today, internal medicine and family medicine physicians comprise the highest number of active specialty physicians. But the number of medical students opting to specialize and sub-specialize continues to skyrocket.
Consider radiology and neurology, two prime areas for sub-specialization. Physicians specializing in diagnostic radiology are trained to diagnose illnesses in patients through the use of X-rays, radioactive substances, sound waves in ultrasounds, or the body’s natural magnetism in magnetic resonance images (MRIs). They can also pursue a sub-specialty in areas such as:
- Abdominal radiology
- Breast imaging
- Cardiothoracic radiology
- Cardiovascular radiology
- Chest radiology
- Emergency radiology
- Endovascular surgical neuroradiology
- Gastrointestinal radiology
- Genitourinary radiology
- Head and neck radiology
- Interventional radiology
- Musculoskeletal radiology
- Neuroradiology
- Nuclear radiology
- Pediatric radiology
- Radiation oncology
- Vascular and interventional radiology
Neurology also offers several sub-specialties, including:
- Brain injury medicine
- Child neurology
- Clinical neurophysiology
- Endovascular surgical neuroradiology
- Hospice and palliative medicine
- Neurodevelopmental disabilities
- Neuromuscular medicine
- Pain medicine
- Sleep medicine
- Vascular neurology
Yet not all of these subspecialties are reflected in the market data surveys. This makes efforts to determine subspecialty compensation particularly challenging.
The Limitations of Market Data
While many subspecialties exist in neurology, radiology, and most other specialties, we know that market surveys do not include all of the specialties above. As physician compensation professionals, we rely on compensation surveys to evaluate compensation in specific specialties and subspecialties. What do you do when there is no market data to reflect a particular specialty or subspecialty?
As robust as the publicly available surveys are, with market data for physicians and advanced practice providers in hundreds of specialties and subspecialties, there are invariably specialties not reported. That’s because there are either not enough respondents in a given subspecialty, or the subspecialty may not be universally recognized. The list of specialties each year typically does get bigger, as shown in Table 1, underscoring the importance of checking for market data annually.
Table 1

Notwithstanding the efforts of market surveys to report a comprehensive list of specialties, no doubt there are occasions where the surveys lack data for the specialty under consideration. Further, while market surveys often include specialties, there may not be data available for certain specialties due to insufficient sample size.
Typically, physicians in a “new” subspecialty possess advanced specialty training, either in the form of a formal fellowship, specific coursework or other training. To assess the premium this level of specialization may warrant, we reviewed reported compensation figures for various specialties and associated subspecialties to attempt to predict the variation in compensation.
This analysis, as presented in the exhibit below, suggests that a premium exists for subspecialty training.
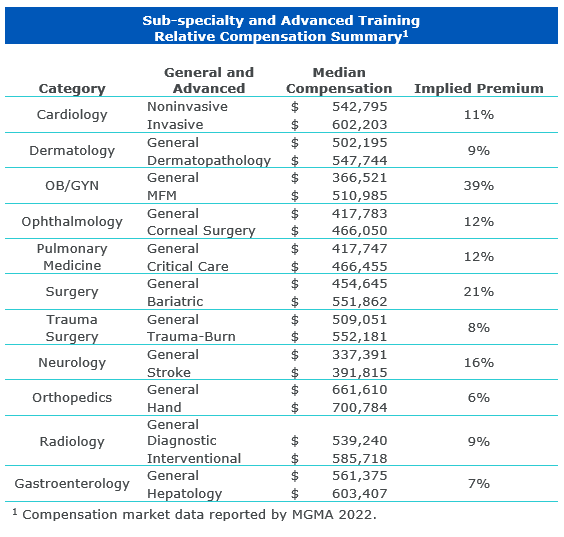
Based on this analysis and our experience, we believe it is supportable to apply a reasonable subspecialty premium to reflect compensation for subspecialties not included in the market data surveys for subspecialty physicians and those with specialty-specific training in advanced procedures.
For example, when trying to evaluate compensation for a gastroenterologist with advanced training in endoscopic retrograde cholangiopancreatography (ERCP) procedures, we may apply a subspecialty premium as follows:
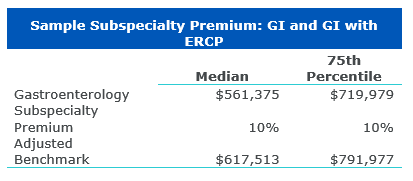
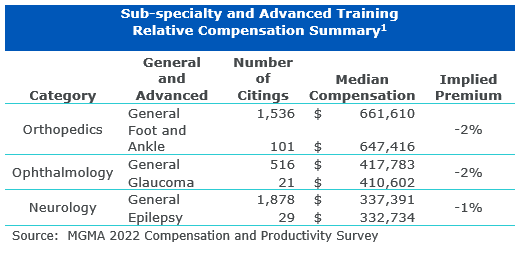
Another challenge in reviewing compensation for super-specialized physicians is that the data may be included in the survey you are using, but the sample size may be so small that the results do not reflect the premium associated with that subspecialty. Take, for example, the following examples, which show a lower cash compensation value for subspecialists. The analyst should be careful not to draw an incorrect conclusion based on low sample sizes.
Determining the Right Approach
Lack of market data or insufficient sample size make it difficult to determine the right compensation for physician subspecialists and super subspecialists. Applying a subspecialty premium and reviewing market data annually is a reasonable approach that can help to retain top talent for the communities your organization serves.
Contact the Author:
Karin Chernoff Kaplan, MBA, CVA, Managing Director, kkaplan@veralon.com