Most current strategic plans appropriately focus on developing capabilities and capacity to support the transition to value-based reimbursement (VBR) as it is anticipated that a decreasing proportion of future reimbursement will be based on fee-for-service (FFS) alone. Uncertainty remains regarding both the pace of and extent to which this transition will occur. Save for the direct impacts of federal health reform (which is focused on ensuring and expanding coverage, though incorporates penalties for relatively low-value care and funds VBR methodology pilots), the transition will be variable by market and influenced significantly by the degree to which a market is payor-centric vs. provider-centric.
It is important to clarify what is generally included in the definition of VBR. More advanced markets (i.e., those in which pure FFS payment is less common) would be unlikely to include pay-for-performance (p4p) in this category, while markets that are more traditional would. Broadly, the only consistent defining factor of VBR is that payment is not based solely on a FFS methodology. If p4p is included on this VBR spectrum, it sits on the far left of the continuum and total cost of care/global capitation on the far right, with shared savings (upside; upside + downside) and bundled payments along the way.
A recently published reimbursement survey(1) indicates that as of 2014, approximately 80% of provider organizations have a mixed FFS/VBR contract portfolio, though the proportion of total revenue, volume, or covered lives represented by contract type is unknown. Among organizations currently under some type of VBR contract, it is clear they anticipate a shift in contract portfolio over the next five years, with an increased proportion of the portfolio to be comprised of VBR contracts. Specifically, these organizations project FFS contracts to represent 34% of 2019 contracts, compared to 57% today.
If FFS represents more than 57% of your contracts today, it may be difficult to imagine a near future in which FFS represents a third of your contracts. There are specific building blocks to prepare your organization for VBR.
Market Influences
First, it is important to understand how your market is positioned relative to VBR. Markets, like organizations, vary greatly in terms of advancement in this area. Many factors influence a market’s progress in VBR, including the positioning of commercial payors and the integration or alignment of the provider community. See Health Strategies & Solutions’ market assessment tool, available within the article “Setting the Right Path and Pace for Integration”, to test the position of your market relative to VBR and other integration metrics.
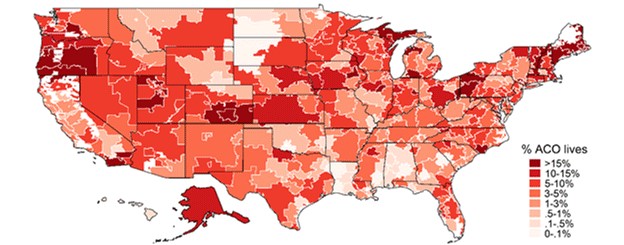
One proxy to show the level of advancement in VBR for a given market is the percent of total lives enrolled in an accountable care organization (ACO). As shown in Figure 1 below, some of the highest areas of concentration in ACO covered lives are in the Northeast and the Pacific Northwest. If you have a low percentage of VBR in a market that is generally less progressive, your impetus for immediate change is less severe. However, if you are in one of the higher concentrated markets in terms of ACO covered lives, change may be coming more rapidly.
Figure 1 – Source: Leavitt Partners Center for Accountable Care Intelligence
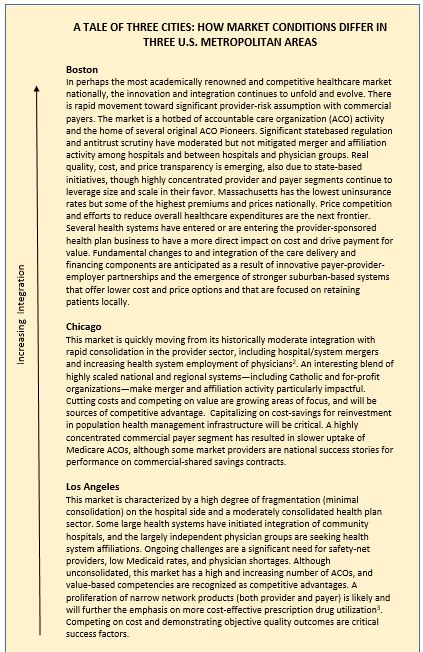
Another proxy to determine your market’s position relative to VBR is integration. Integration (provider + provider, provider + payor, etc.) is a hallmark of a progressive provider-payor market and one that is likely to be more advanced in VBR. Health Strategies & Solutions has completed a comparative profile of three metropolitan areas in the United States (see below). A similar evaluation can provide insight as to where your market is or may be moving in terms of VBR.
Figure 2 – Profiles of Differing Market Conditions in the U.S.
Building Blocks Towards VBR
If you have a very low percentage of VBR today, there are many building blocks that can help your organization to succeed as the environment continues to transition in this area over the next several years. Several of these potential building blocks are listed below:
- Measure outcomes, demonstrate success– The ability to measure clinical outcomes and, more importantly, demonstrate results to outside parties is a key first step in moving towards VBR. There are minimum information system requirements to track clinical outcomes; however, basic metrics can be measured by virtually every provider organization without significant technology barriers. Once outcomes can be demonstrated, payors and other providers will be willing to discuss pilot programs in VBR.
- Prepare your employed physicians– Physicians are important stakeholders in the transition to VBR and, as with any major change, some level of resistance is to be expected. Health system employed physicians are better candidates to initiate this transition than lesser aligned community physicians. Incentivize employed physicians to manage costs and improve clinical outcomes and service quality with some portion of compensation tied to these defined metrics. The percentage of compensation at risk for value should exceed the percentage reimbursed by payors, to create incentives for serious attention to value.
- Identify specific conditions for clinical pathways management– Successful chronic disease management is important to success in VBR. Select several prevalent diseases to standardize care processes to ensure successful outcomes and low costs.
- Assume full risk for your own employees– Many health systems have a population available to manage costs and outcomes – its employees. Being self-insured allows an organization to manage population health on a smaller scale before expanding to a broader segment of the community.
No matter where your organization is along the spectrum of VBR, it is never too soon to plan for the future. It is still largely a FFS environment today, so your strategies and metrics must reflect this reality in terms of focus and resources, especially in the near-term. You’ll need to understand your organization’s position and market to transition to VBR at the pace and degree that will ensure success – not just today, but in the years to come.
Footnotes:
(1) McKesson Health Solutions. The State of Value-Based Reimbursement and the Transition from Volume to Value in 2014
(2) http://www.northshore.org/newsroom/press-releases/northshore-advocate-merger/