by Lynda Mischel, Principal
and Scott Stuecher, Manager
Open PDF file >
Radiation Oncology Alternative Payment Model: 3 Things to Do Now
CMS is launching a Radiation Oncology Alternative Payment Model (“RO Model”) that will profoundly affect radiation oncology economics, with a target start date of January 1, 2022. The RO Model will apply (or at least test) a bundled payment methodology affecting about 30% of eligible radiation oncology episodes. Revenue reductions may be as high as 25% for the traditional Medicare population in conventional radiation and as high as 40% in the 30 proton therapy centers nationwide.
Many predict that the RO Model will further shift care toward hypofractionation which requires fewer treatment sessions. However, the clinical protocols continue to be developed in many disease sites and require further investigation.
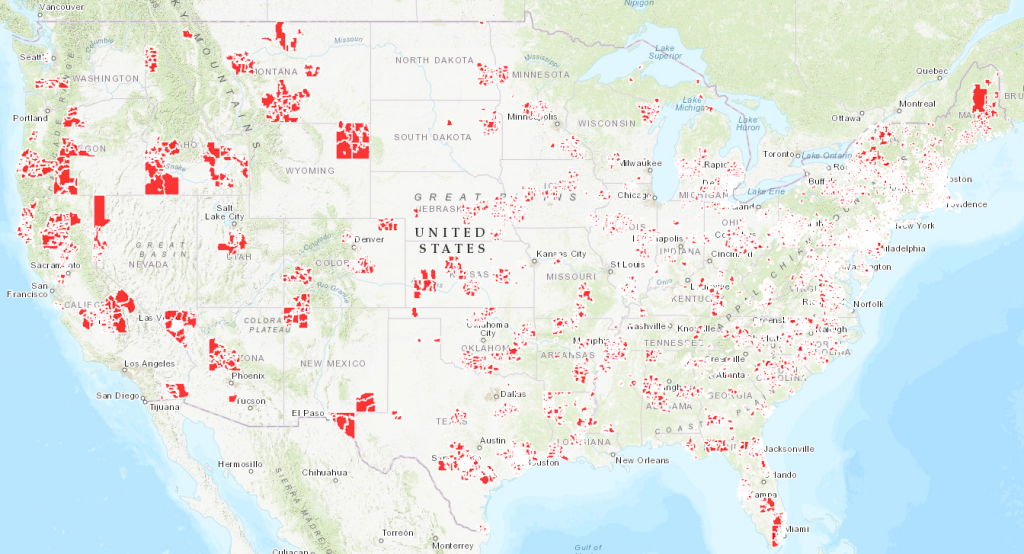
As indicated in the map below, CMS has identified specific markets in which the RO Model will apply.
Each center in an identified market needs to:
- Understand the RO model impact on revenue
- Prepare for the new reporting and billing requirements
- Pursue opportunities to build capacity
RO Model Participating Zip Codes
To check if your program is in an RO Model zip code, view this file.
Understand the RO Model Impact on Revenue
Each radiation and proton therapy program is unique, with a specific disease, age and payer mix. In order to develop a plan, a program needs to analyze the volume of patients by disease, number of fractions and payer mix preferably over several years of operation. This volume analysis will assist in forecasting the reimbursement, under the RO Model. The forecasting exercise will yield estimated reimbursement by disease site, ultimately leading to an adjusted revenue estimate. This analysis also may assist in identifying options to increase capacity by identifying opportunities for hypofractionation by disease site. The final adjusted revenue should also reflect the adjustments, withholding and potential reconciliation dollars from the bundled payment.
Prepare for New Reporting and Billing Requirements
The RO Model has significant new requirements for reporting and billing. CMS is supposed to supply each center with its specific payment factors including a trend factor, geographic adjustment, case mix, historical experience and an efficiency adjustment. All of this leads to a bundled payment by disease site which must be billed using the RO Model specific HCPCS code. Each participant needs to evaluate the capacity of the oncology information system and billing system to process these changes for the specific population.
The new RO Model also includes a quality reporting requirement. The four direct quality measures must be reported for the entire patient population. Moreover, CMS will require specific clinical information on Medicare recipients with specific diseases. Many radiation oncology programs do not currently report specific quality data and may not have automated capabilities in the oncology information or the medical records systems to assure appropriate documentation and reporting.
Pursue Opportunities to Build Capacity
The shift to a single bundled payment for each patient is likely to encourage faster innovation and research in hypofractionated treatment which involves fewer treatments (or fractions) for each patient. This trend has been happening in radiation oncology for some time, especially in specific disease sites like brain and prostate. Many organizations in conventional radiation therapy and proton therapy have been researching and increasingly treating patients using new, shortened hypofractionation protocols. Moreover, new technologies are under investigation that will also affect length of treatment. Clinical teams across the country, both in and out of the RO model, should carefully evaluate the benefit of hypofractionated treatment for patients and consider the impact this will have on facility capacity.